
SPECIALIST ENDODONTIST IN MERSEYSIDE
The Sandstone Dental Practice welcomes endodontic referrals for private root canal treatment. With our highly experienced team, we can accept referrals for more complex cases. Our team includes a specialist endodontist in Merseyside and a dentist with a Special Interest in Endodontics, and we have treated a large number of difficult cases referred to us by our clinical colleagues in Merseyside and beyond.
ENDODONTIC SERVICES AT THE SANDSTONE DENTAL PRACTICE INCLUDE:
- Skilled diagnosis, treatment and management
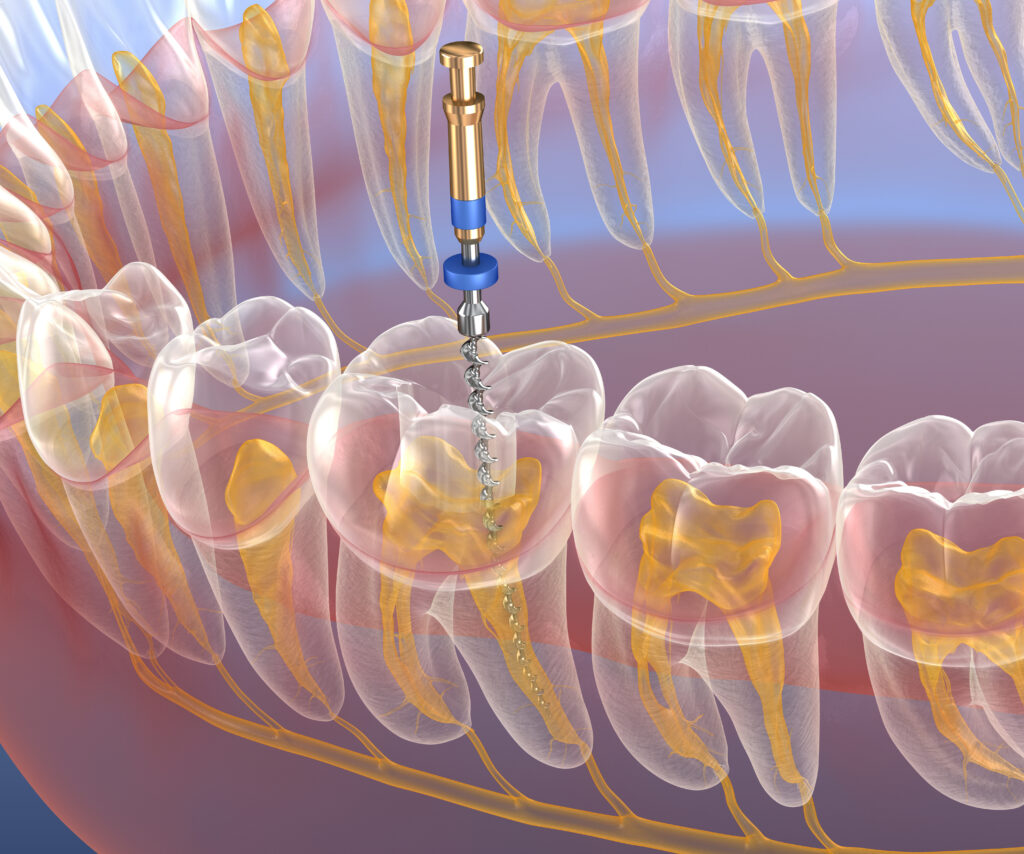
- Root canal treatment and retreatment, using a dental operating microscope
- Internal bleaching and inside outside bleaching for treatment of dark teeth
- Management of dentoalveolar trauma
- Endodontic microsurgery undertaking using the dental operating microscope
- Management of resorption defects and dental anomalies
REFER YOUR PATIENT FOR HIGH-QUALITY ENDODONTIC TREATMENT IN THE WIRRAL, CHESHIRE AND MERSEYSIDE
If you would like to refer your patient to The Sandstone Dental Practice for root canal treatment, you can be assured that your patient will be in very experienced hands. Our team will assist with all aspects of your patient’s treatment, from planning and preparations through to follow-up appointments, and you are welcome to accompany your patient at any stage of the treatment process. Once treatment is successfully completed, the patient will be returned to you for continued care at your practice.